Two days ago after a typical day performing procedures in the EP lab, doing inpatient consults, fielding patient messages, attending administrative and research meetings, reading EKGs, Holter monitor recordings, and co-signing device clinic charts, I opened my email and saw this:
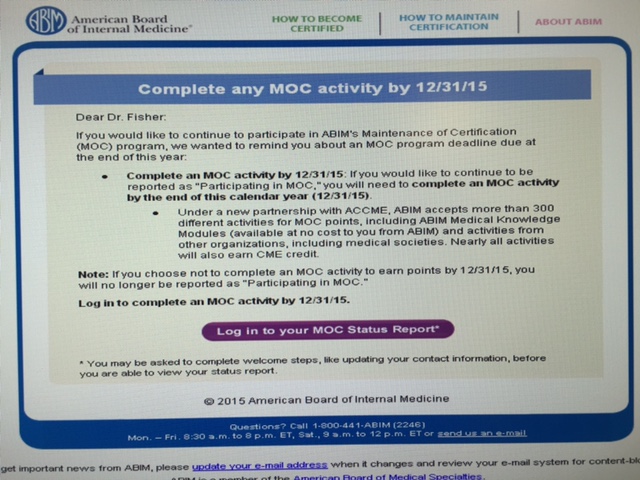 |
| ABIM Email to Diplomats 11/20/2015 |
I was appalled. MOC is not longer about "keeping up" for physicians. It is a major distraction. This program is of unproven benefit to my patients and me. Thanks to haphazard and self-serving rule changes by the ABIM and their member boards over the past 25 years, the US Specialty Board system has become increasingly coercive. In fact, MOC program now threatens my ability to practice the work that I love because I could lose my facility privileges and ability to receive payments from insurers on December 31, 2015. That is my reality. This is the reality of every physician subspecialist who participates in the ABMS MOC program in US medicine today.
Remarkably, I just re-certified in Cardiovascular Diseases and Cardiac Electrophysiology in 2013
for the third time. I have never failed. I have over thirty years of experience treating patients and standing in the cross hairs of what it means to be truly accountable to those I treat. I have had over thirty years of nights when I lie awake at night worrying about by patients, about if I did enough, about why a patient had to die. My family, too, has endured years of being woken in the middle of the night or seeing their father have to leave a school play, holiday concert, or friend's dinner party to place an emergency pacemaker.
I am not unique. I am a practicing physician everyman. I stand in unison with hundreds of thousands of others here in the United States just like me who get up every day, kiss their loved ones, and head off to do their favorite job in the world - a vocation so completely immersive and rewarding that we gladly give up a part of ourselves to earn the trust and faith of our patients and fellow physicians.
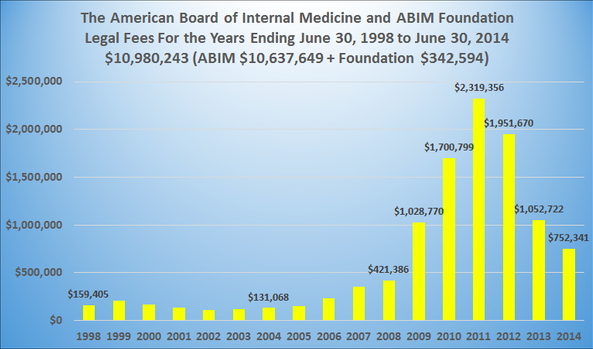
And because I've been practicing medicine so long, I know I do not need a private, unaccountable, and irresponsible organization to tell me how to behave. I am better than that. After experiencing the busywork of the evolving MOC program and its lack of value for the time spent, I looked into the corporations who promote this exercise. I had the help of accountants and fellow physicians who were similarly upset and uncovered a vast array of hidden financial activities of the ABIM and their collaborators. There is so much financial corruption it is mind-boggling. The conflicts of interest that are never acknowledged and corrected make my stomach churn. The practice of medicine is better than this. Practicing physicians are better than this. We do not need some dystopic corporate Big Brother watching over us to assure we log into a computer every so often to enter data that can be used against us. We do not need webcams, video monitors, body inspections, keyboard tracking, and palm scans to prove we are honest and ethical and won't cheat on examinations. But this is what the ABIM has become: some new form of quasi-police state for monitoring physicians.
Working in fear is not what I want for medicine. It certainly is not how I want my youngest colleagues to grow up learning and practicing medicine. But the ABIM and their parent organization, the American Board of Medical Specialties (ABMS), seem to love fear, humiliation, and intimidation to get doctors to participate in their lucrative MOC program. It is sickening. It is also the height of hypocrisy for these organizations to claim to run an organization that attempts to "Choose Wisely" when that same organization funnels tens of millions of dollars for itself from hard working physicians so they can choose an investment portfolio with multi-million dollar condos, meet at swank meeting venues, pay for spousal travel fees and first class airfares as they preen themselves in front of media lights. The ABIM Foundation "created to define medical professionalism" for the public? Give it a break.
Rest assured I am not naive. I know how important this MOC program is to certain investors. As I peel back layer after layer of the interconnected workings of these ABMS member boards and the ACGME, I know how high this MOC program goes and how dark this MOC program and its tactics have become. I completely understand that these specialty board organizations have managed to wedge themselves into our new health care law that calls itself "Affordable," wedged there by undisclosed lobbying efforts funded by the very doctors whose blinded trust was violated beyond comprehension. Just because these corporations want to make a buck.
So let me take the stick a moment. Let me be perfectly clear and I don't say this lightly. I'm sure I say this on behalf of tens of thousands of other hard-working, honest, and ethical physicians. We have had enough of the ABIM and the ABMS MOC program. It is time to end it -
completely. No more "modifications" to make this broken program "easier." No more "listening" to our concerns but continuing this failed experiment. No more "MOCA Minutes" that we have to turn our gaze from our patients toward the computer screen or iPhone even longer. Continuing the ABMS MOC that has proven itself to be morally and financially corrupt, and exceedingly expensive to physicians, patients, and our health care system is ill-advised for our profession. The conflicts of interests alone are worth hundreds of millions of dollars to the corporations that stand to make millions from physician assessment, yet we never hear a word about this from them ABMS or the ABIM on this reality.
I am better than how the ABIM and ABMS threaten to label me. I served this great country for twenty-six years as a physician with the United States Naval Reserves and I continue to work every day to make sure I do the best I can for my patients in this increasingly difficult health care delivery environment. I worked then and work now beside hard-working corpsman, nurses, administrators and technicians who don't want to rock the boat and just want to do what's needed to finish our job every day. These people and the patients I care for are why I go to work every day.
So I ask the leadership of the ABIM: "Why does the ABIM insist on placing a "scarlet A" on my reputation by labeling me a "Not Participating in MOC?" Such labels are offensive. I participate in ACGME-accredited CME as required by my license to practice medicine in the State of Illinois. I am not a slacker. I teach residents and fellows, for goodness sakes. I am certainly not one who doesn't mind working hard. I am a proud practicing physician with more years of clinical experience and direct patient care than any of you.
Please don't be libelous and cast aspersions my way with your on-line labels. I've got much more important things to deal with. Stop pretending that you speak for "the public" and know what's best for them in health care when you don't even crack the door of an examination room or know what I do. Proceeding to take away my hard-earned reputation and ability to practice medicine because of your little label is both threatening and hugely upsetting.
Think about these words. Think about them carefully.
I beg of you and your affiliated private organizations to stop the labels.
The profession of medicine is better than this.
Your everyman,
Wes