Yesterday was a remarkable day for practicing US physicians. It was the day two articles appeared side by side in the
New England Journal of Medicine: one
promoting the American Board of Medical Specialties' Maintenance of Certification® (MOC) program, and another that
thoroughly debunked it. The comments placed to the stories told a story of solidarity, pent up rage, of corruption within our profession, and a commitment to change the status quo. Doctors were
relieved to learn that an alternate pathway to MOC, the National Board of Physicians and Surgeons, might offer a slightly less expensive pathway to acquire MOC points.
But I worry physicians might be reacting, rather than carefully considering, the implications of the alternate proposal.
I should say that I applaud Dr. Paul Tierstein's phenomenal piece
published yesterday in the
New England Journal of Medicine. He cogently articulated the many problems with the ABMS MOC program but stopped short of dismantling the ABMS (and ABIM's) board re-certification process entirely as he
promoted his new "National Board of Physicians and Surgeons instead:"
There will be three or four requirements, and you have to be certified by an ABMS board initially. We're not taking that on. I think the fellowship process is great, it's like a final exam for residency and fellowship. I think most people agree that it's okay (not perfect, but okay). You'll also have to have a valid medical license and not to have been denied privileges recently in your specialty. Then the key requirement is 50 hours of continuing medical education, provided by an ACCME-accredited provider over 2 years. And the cost will be far lower. The cost will be as little as possible.
While this may be an acceptable solution to the current MOC conundrum created by the inclusion of ABMS and the MOC program in our new health care law, I believe we should first investigate how the ABMS and MOC program became part of the Affordable Care Act in the first place.
Troubling concerns of collusion of ABIM board members with the Center for Medicare and Medicaid Services (CMS) and the National Quality Forum (which receives the bulk of its revenues from grants supplied by CMS) exist. Christine Cassels, MD, who is the current President and CEO of the
National Quality Forum, was President and CEO of the ABIM from 2003 to 2013 and ultimately responsible for the
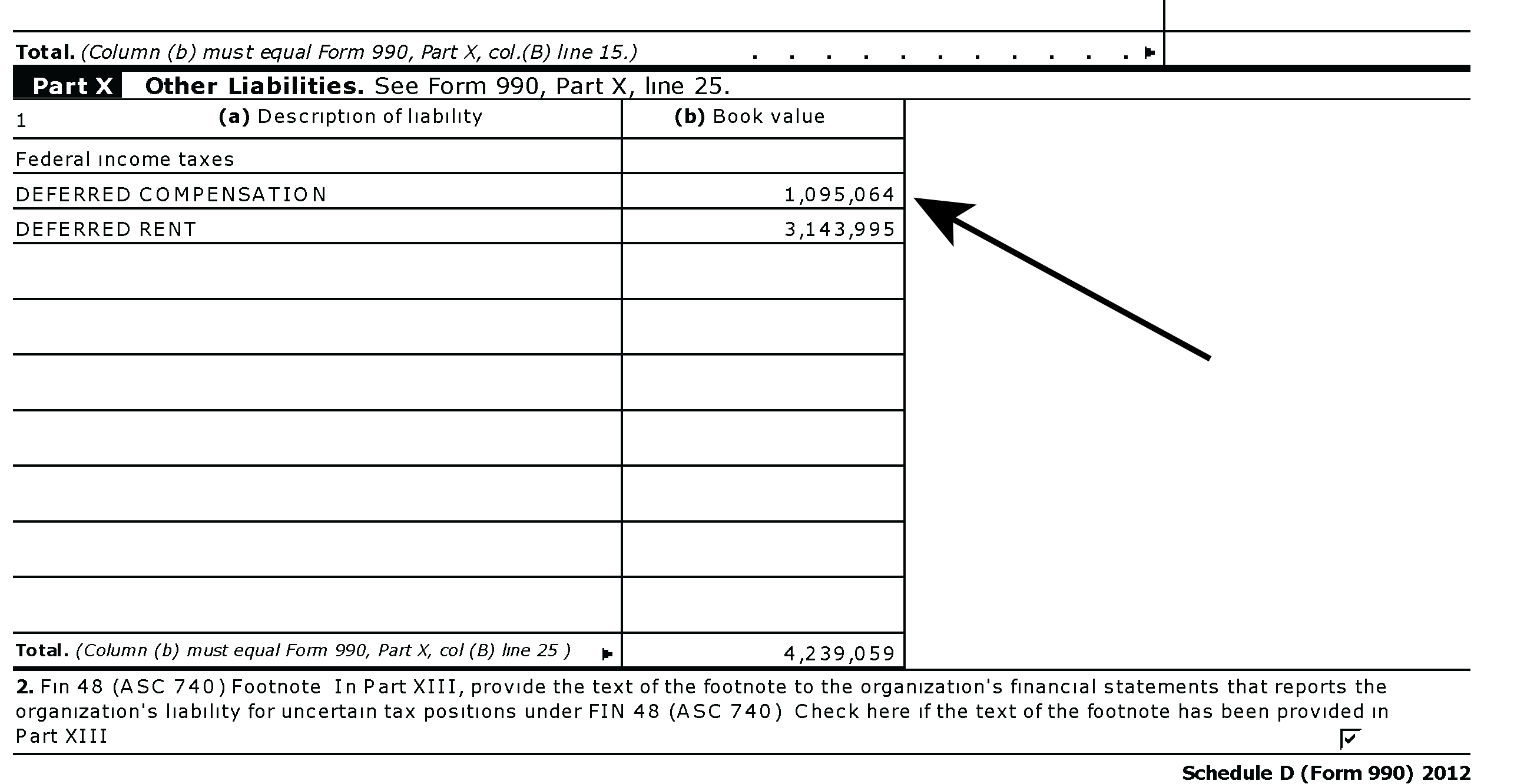
$2.3 million dollar luxury condominium purchase by the ABIM Foundation in December, 2007. Richard Baron, MD served as treasurer of the ABIM and later an unpaid Director of ABIM in 2007-2008. Dr. Baron also served as Group Director of Seamless Care Models at the CMS Innovation Center which
claims it "Identifies, validates and disseminates information about new care models and payment approaches to serve Medicare and Medicaid beneficiaries seeking to enhance the quality of health and health care and reducing cost through improvement." Dr. Baron then became a full-time employee of CMS in 2011-2012 before returning to ABIM in 2013.
Which leads to the question: how much influence did the ABIM leadership have in establishing a continuous money stream for itself and its Foundation during the writing and mark-up of the
Affordable Care Act? (see pages 247 and 844-845 of this large pdf). Clearly, there should be public record available to this effect and physicians should inspect this record before creating an alternate MOC pathway.
Because if the ABIM influenced the writing of the Affordable Care Act for its own enrichment, rather than for "public good," this represents further corruption of an already broken MOC model, in my view. There have been many experienced physicians adversely affected by the current MOC program.
So these are the questions practicing physicians should ask before enrolling in the current, or any other, MOC pathway:
(1) Do we need MOC at all? and
(2) Don't we need a full public disclosure of the audited financials of the ABIM and the ABIM Foundation and their financial dealings first? and
(3) Shouldn't we insist on removal of the corrupt MOC program entirely from the changes made to Social Security Law by the Affordable Care Act before creating another unaccountable organization to practicing physicians?
-Wes






{kind=link}
{kind=link}